Healthcare Respirator Programs During (and After) Covid
February 28, 2021
For many healthcare employers, the Covid-19 pandemic was the beginning of a workplace respirator program. Most did not have a respirator program prior to the pandemic, and are looking forward to returning to that, but aren't sure how to make that decision moving into 2021.
Without a fairly detailed dive into the specific of your workplace, existing safety policies, types of procedures performed, patient screening methods used, regulations specific to your healthcare sector, and a variety of other risk factors, we cannot advise on a specific course of action. For employers looking for professional guidance of this type, we offer consulting services and can provide a proposal.
For healthcare employers making this determination themselves, they should carefully review Cal/OSHA's Aerosol Transmissible Diseases regulation, California Department of Public Health requirements, and any local City/County guidelines, and consider the following:
Will employees be seeing confirmed or suspected Covid-19 patients?
If you are, for example, a medical clinic that will be seeing patients with respiratory or flu symptoms for evaluation and diagnosis, or you are a dental office that will have to provide emergency care for patients who have Covid 19, Cal/OSHA's aerosol transmissible diseases standard requires a full respirator program (with fit testing and training renewed annually).
If you are not seeing confirmed or suspected Covid-19 patients, conduct screening of all patients (recognizing fully the limitations of symptom and history based screening methods that will not detect asymptomatic and presymptomatic individuals), outpatient medical and dental offices have greater leeway in determining whether to continue with a respirator program.
One important point is the nature of healthcare often requires providing urgent or emergency care to patients who may either have Covid-19, or have other fairly common upper respiratory symptoms that would meet the criteria for potential Covid-19 infection.
Will employees be required to wear a respirator? Remember: an "N95 mask" is a respirator.
Regardless of risk, if employees are required to wear a respirator for any work tasks, you must implement a full respirator program (with fit testing and training renewed annually).
Are there other regulations or third party standards requiring a respirator program?
Even though you may not be required to maintain a respirator program by Cal/OSHA requirements, there may be public health requirements specific to your industry that require it. Or, third party organizations may require it as part of their accreditation standards.
Even though you may not be required to maintain a respirator program by Cal/OSHA requirements, there may be public health requirements specific to your industry that require it. Or, third party organizations may require it as part of their accreditation standards.
How has the availability of vaccination changed risk factors in the workplace?
There is always a benefit from decreased community transmission, but the impact on vaccination programs in your specific organization depends on a variety of factors, including the willingness of your workers to take the vaccine (and, related, your company policy on requiring them as a condition of employment). Significant ambiguity still exists regarding the duration of protection offered by the vaccine, and its effectiveness against emerging variants of Covid-19.
Is a respirator program needed for other pathogens?
Many employers have discovered that even with a decreasing threat from Covid-19, they still have a need for a respirator program (and in fact, should have had one all along). Particularly within medical clinics and hospitals, there may be a need to protect certain classes of employees from pathogens like tuberculosis. Dental professional may have to provide emergency care to a patient who also has a respiratory illness, and need a higher level of protection than would be provided by a procedure mask.
How effective are other safety controls used in the workplace?
Personal protective equipment like a respirator should be used when there are not other ways to effectively manage a hazard. Safer work practices and engineering controls, like isolation shielding or air purifiers, should be the first line of defense. The more effective these methods are, the less need there is for a respirator. Unfortunately, quantifying the effectiveness of controls against biological contaminants is not as easy as it is for chemical contaminants (where a variety of well-established methods exist to measure airborne concentrations)...so there's a fair amount of research and more qualitative professional judgement required here. A lack of effective safety controls, or ambiguity about their effectiveness means a respirator program should be maintained.
Would a respirator program, even if not required, improve workplace conditions?
Just as they did in early 2020, many employers deciding they will continue to maintain a respirator program through 2021 for all clinical staff, to keep everyone as safe as possible, which paid dividends in terms of morale, employee retention, and job satisfaction in the midst of the pandemic. There are also benefits in terms of reduced workforce disruption (less need to quarantine employees with potential exposure if they are wearing appropriate protective equipment).

Respirator facepieces, cartridges, and filters are routinely counterfeited. Most buyers cannot verify whether what they received is authentic, and the marketplace isn’t set up to ensure authenticity. Respiratory protection is especially vulnerable to counterfeits because the most safety-critical functions cannot be confirmed by visual inspection. A trained eye might catch subtle tells, inconsistent molding marks, off-color materials, or printing and labeling errors. But appearance does not verify performance. You cannot reliably determine by sight whether a cartridge contains the correct sorbent, whether a particulate filter actually meets its required performance rating, or whether facepiece materials and components will maintain a stable seal under real-world conditions over time. A respirator’s protective performance is driven by materials and manufacturing tolerances, including the composition and consistency of the facepiece elastomer, the integrity of the lens and frame, strap and buckle hardware strength and elasticity, sealing surface geometry, and the design and quality of inhalation and exhalation valves. Small substitutions or dimensional changes can materially affect fit, seal reliability, and durability. For filter cartridges, protection depends on the correct filter media or sorbent formulation, a reliable seal between the cartridge and the facepiece, and internal construction that controls airflow distribution and loading. Substitutions in media, sorbent, adhesives, gaskets, or internal geometry can reduce protection immediately and may lead to premature chemical breakthrough or inadequate filtration performance. Because these performance characteristics cannot be confirmed by inspection, the only practical safeguard is a verifiable supply chain. When chain of custody is unclear, the buyer has no defensible basis to trust authenticity, certification, or performance. The risk is highest when products come from online marketplaces like Amazon, especially third-party sellers, liquidators, or “new in box” resellers with no traceable sourcing. Commingled inventory practices, where “identical” products from different sellers can be pooled in warehouses, further increase the risk of counterfeit products entering the supply chain. Despite specifically advising clients not to purchase PPE, especially respirators, from Amazon, eBay, or similar online marketplaces, we are seeing this guidance disregarded. We arrive to fit test respirators that show subtle differences from the authentic 3M products we supply. In multiple cases, those units are ultimately confirmed as counterfeits purchased through the exact sources we advised against. Using price as the primary, or only, selection criterion for a personal protective equipment vendor is irresponsible. The employer owns the consequences of negligence in purchasing. If there’s an exposure incident, an injury, or an audit, “we got it online” or "it had free Prime shipping" is not a defense. Workers notice too. When employees don’t trust the gear, company safety culture quietly collapses. Buy PPE through: - Authorized distributors - Direct from the manufacturer - Established industrial or safety suppliers with traceability
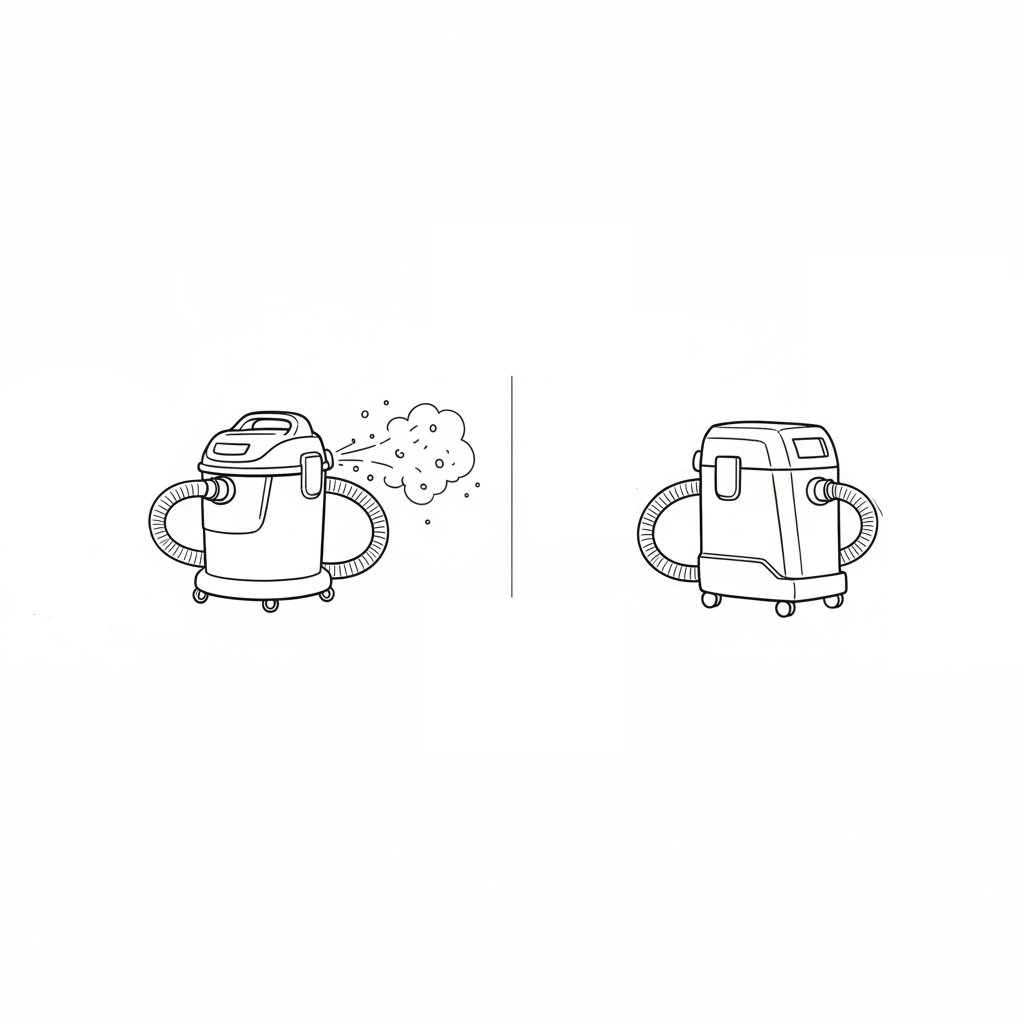
At a glance, a shop vacuum with a HEPA filter and a dedicated HEPA-rated dust extractor might seem to do the same job: collect dust and debris. In reality, the difference between them is substantial, especially for fine particulate control, worker protection, and regulatory compliance. Adding a HEPA filter to a standard shop vacuum improves filtration, but it doesn’t turn the unit into a true HEPA-rated system suitable for hazardous dust. Key takeaway: If you’re collecting fine dust from hazardous materials, use an extractor designed and certified for that purpose. Don’t rely on a shop vac with a retrofit HEPA filter. Here’s why: Most shop vacs leak around seals or bypass fine dust through motor vents, even if they use a HEPA filter. A proper dust extractor is designed from the ground up for fine dust control. All seals, gaskets, and joints are engineered to prevent leakage, and the entire system, not just the filter, is tested to meet HEPA performance. Shop vacs are built for high pulling force (static pressure) to pick up debris, nails, or sawdust through hoses. Dust extractors are designed to steadily move larger volumes of air (airflow) and catch fine, respirable dust particles before they disperse. Shop vacs clog quickly when used on fine dust; when the filter clogs, vacuum pressure drops, and more dust escapes into the air. Dust extractors include self-cleaning or pulse-clean mechanisms that shake accumulated fine dust off the filter. This leads to consistent pressure levels, and extends filter life. A shop vac is meant for short-term cleanup. Dust extractors are designed for longer periods of use, often with features like automatic tool-start functions, variable speed control, anti-static hoses, and spark-resistant motors for combustible dust safety. For operations covered under Cal/OSHA or Federal OSHA silica standards, or for controlling other hazardous respirable dusts like carbon, graphite, metals, wood, or asbestos, a simple shop vac with a HEPA filter is not sufficient. Hazardous materials require commercial-grade HEPA-filtered dust collection systems engineered and tested for fine particulate containment and exposure control.
Respirator cartridges for gas or vapor protection have a limited service life. They need to be changed before they become saturated and can no longer purify the air effectively. If an employer is using air-purifying respirators for protection against gases and vapors, Cal/OSHA T8 §5144(d)(3)(C) requires that the employer either: Use a cartridge with an end-of-service-life indicator (ESLI) that provides an indication to the user that the cartridge has reached the end of its service life. Unfortunately, ESLI cartridges are not available for most chemicals. Implement a time-based cartridge changeout schedule. This must be, per Cal/OSHA, “based on objective information or data that will ensure that ... cartridges are changed before the end of their service life. The employer shall describe in the respirator program the information and data relied upon and the basis for the ... cartridge change schedule.” Relying on users to detect the end of the cartridge service life by smell, taste, or irritation of the chemical passing through is not compliant as a primary method for cartridge changeout. It may be used only as a secondary safeguard to the employer's time-based changeout schedule. This is a common mistake: an employer identifies a potential respiratory hazard, buys respirators, and provides fit testing - yet skips the crucial step of a formal, documented hazard assessment and changeout schedule. For gas or vapor exposures, your written program should clearly specify: • The correct respirator type for the task • Appropriate cartridge or combination filter-cartridge • A time-based changeout schedule supported by data Safewest can help develop or review your respirator program, including hazard assessments and cartridge change schedules. Contact us to make sure your program is compliant and your employees are protected.
HAZWOPER (Hazardous Waste Operations and Emergency Response) training requirements apply to certain operations involving hazardous waste. These requirements dictate the amount, type and levels of training that employees working with hazardous waste must receive. The requirements for hazwoper training can be found in Cal/OSHA § 5192 and Federal 49 CFR 1910.120 . In general, there are three categories of hazmat operations, and specific training requirements for each. These three categories are hazmat site cleanup, emergency response, and operations at treatment, storage, and disposal (TSDF) facilities. Site Cleanup Cleanup and removal work at sites that have been identified by a government agency (state, federal, or local) as having an accumulation of hazardous substances that creates a threat to the health and safety of individuals or the environment or both. General site workers removing hazmat with potential exposure to hazardous substances and health hazards shall have 40 Hours of Training + 3 Days Supervised Field Experience. General site workers in areas where hazard levels have been fully identified, exposures are below published safety limits, there are no health hazards, no possibility of an emergency release, and respirators are not required shall have 24 hours of training + 1 day supervised field experience. Occasional/limited site workers (such as those doing monitoring or surveying) and are unlikely to be exposed to dangerous levels of hazmat shall have 24 hours of training + 1 day supervised field experience. Supervisors of general site workers shall meet the same training requirements as that category of general site worker, plus have an additional eight additional hours of specialized hazardous waste operations management training. All categories of site cleanup workers shall have 8 hours of annual refresher training. Emergency Response Emergency response to releases of, or substantial threats of releases of, hazardous substances, regardless of location. Awareness Level (FRA): Basic awareness, recognize hazmat threat, call for help. Competence based, no hourly requirement. Operations Level (FRO): Defensive response, contain and limit the release. 8 hours of training required (or a competence-based option exists for experienced workers). Hazmat Technicians and Hazmat Specialists: Direct response to stop a release of hazardous substances. Training scope and duties varies depending on position/role. 24 hours of training required. Incident Commander/Manager: Control and manage scene, implement response plans. 24 hours of training required. All emergency response workers shall receive annual refresher training or evaluation to demonstrate competency in their required areas. TSDF Operations Operations at Hazardous Waste Treatment, Storage, and Disposal Facilities (TSDFs) Workers are required to have 24 hours of initial training, and 8 hours annual refresher training.